Papers relating to the pituitary body, hypothalamus and parasympathetic nervous system / [Harvey Cushing].
- Cushing, Harvey, 1869-1939.
- Date:
- 1932
Licence: In copyright
Credit: Papers relating to the pituitary body, hypothalamus and parasympathetic nervous system / [Harvey Cushing]. Source: Wellcome Collection.
192/254 (page 178)
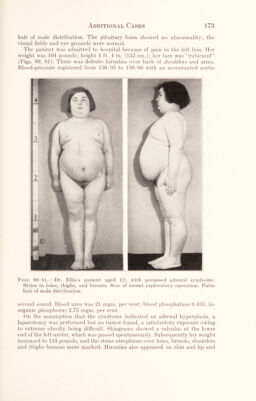
![The anaesthetic had been given by Dr. W. M. Boothby with the Connell apparatus and was smoothly taken. The operation lasted just short of three hours and at its conclusion the patient was in good condition and there seemed to be no reason to expect anything other than an uneventful recovery. Subsequent notes.—On first regaining consciousness (1:30 p.m.), while still in position on the operating table, the patient complained of feeling chilly and of abdominal discomfort. He vomited more than usual (a bile-stained fluid) and his bowels moved freely, the stool containing mucus streaked faintly with blood. After he was removed from the table at 3:30 p.m., he complained of in¬ creasing abdominal pain; the belly seemed somewhat stiff and tender to palpa¬ tion but no especial significance was attached to the fact. During the rest of the afternoon, he continued occasionally to retch, vomit, belch and pass gas per rectum. He had also a peculiar grunting expiration which, however, was regular and without Cheyne-Stokes’ rhythm. He was finally taken to the ward at 6 p.m. His rectal temperature was then 102.4°. Owing to restlessness and further complaints of abdominal pain, he was given at 8:30 p.m. a sixth of a grain of morphia subcutaneously. Not long after this his pulse and respiration began to quicken and at 10:30 p.m. to quiet him he was given another one-sixth of morphia. From this time onward he became progressively worse; at 1:00 a.m. his rectal temperature was 104°. His appear¬ ance an hour later, when I was called to see him by my then assistant, Dr. E. B. Towne, reminded me of a state of “hyperthermic shock,” whatever was meant by that. My personal notes state: “2 a.m. He is conscious, alert and subjectively com¬ fortable but breathing rapidly with an expiratory grunt; no rhythmicity about respiratory act; pulse very irregular, often barely perceptible and uncountable at the wrist. Extremities cold and clammy though he says they feel hot.” And again at: “5 a.m. Has slept off and on the past three hours on his mor¬ phia. No change in general condition. Has voided. Difficult to tell what is wrong. He is mentally clear and cheerful. The abdomen is slightly distended and so sensitive it cannot be touched without making him wince. This superficial tenderness suggests some spinal cord (referred pain) complication. To exclude the possibility of a postoperative clot a lumbar puncture has been made. Fluid found clear and not under tension.” “6:30 a.m. Definitely failing though remains conscious and clear. Pulse barely perceptible. The condition now looks more like a general peritonitis as from a perforative ulcer, a mesenteric thrombosis, or acute obstruction (though no vomiting since morphia) than any intracranial condition with which I am familiar.” He grew increasingly worse, became cyanotic and nearly pulseless and the end came at 10:15 a.m., just twenty-four hours after the start of the operation. [It was subsequently learned from the patient’s wife that on the day before his operation he had eaten some cake, brought to him by a visitor and this had disagreed with him. Indeed, so long as she had known him, he had aways had a poor digestion and would frequently regurgitate food “like a baby with an overfilled stomach.” In 1903, he had had an atack supposed to be appendicitis with “stoppage” from which he had recovered without operation after discharging some dark material by the bowel.] Post-mortem examination (Dr. J. L. Stoddard).—The unrestricted autopsy was held at 1:15 p.m., three hours after death. Apart from the recent operative](https://iiif.wellcomecollection.org/image/b2982221x_0192.jp2/full/800%2C/0/default.jpg)